- Use of opioids—Massachusetts
- Hospitalizations—Massachusetts
- Deaths—Massachusetts
- Massachusetts Overdose Prevention Strategy
- Massachusetts Opioid Abuse Prevention Collaborative
State-level estimates of heroin use are often difficult to obtain because few surveys include present findings specific to heroin. Some national surveys may collect data on heroin users but then don’t provide results separately by state.
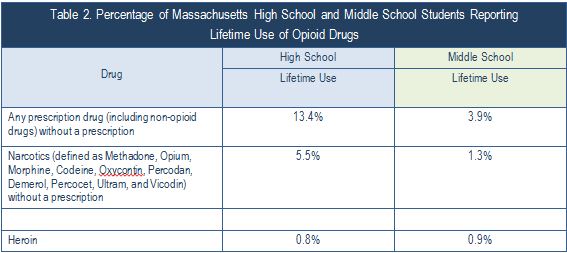
Data on the use of opioids by high school and middle school students are available from the Massachusetts Youth Health Survey (YHS) conducted by the Massachusetts Department of Public Health. According to the 2013 YHS (see Table 2), approximately 13% percent of Massachusetts high school students report nonmedical use of prescription drugs (which include opioid drugs) in their lifetime, 5.5 percent report nonmedical lifetime use of narcotics, and 0.9 percent report having used heroin in their lifetime. Middle school students are less likely than high school students to use these substances, 3.9 percent report nonmedical use of a prescription drug in their lifetime, 1.3 percent report lifetime use of narcotics, and 0.9% report lifetime use of heroin.
Estimates of the misuse of prescription opioids in Massachusetts are also available from the NSDUH survey. According to the 2012 and 2013 NDSUH, about 3.7 percent of persons ages 12 or older in Massachusetts report using pain relievers nonmedically in the past year. Misuse of pain relievers was most common among young adults ages 18 to 25 (8.5%) compared to those ages 12-17 (4.1%) and those ages 26 and older (2.8%).9
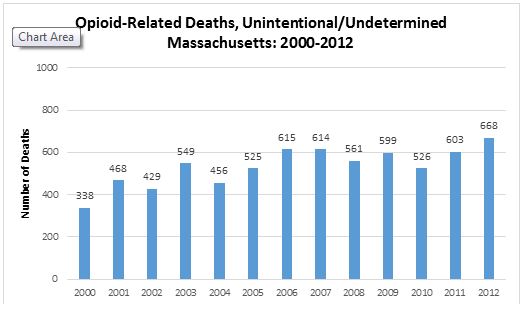
Considering that the rate of fatal overdoses in Massachusetts has increased significantly in the past 15 years (see graph below), prevention strategies that target all opioids (heroin as well as prescription opioids) are particularly important at this point in time.
Hospitalizations—Massachusetts
- Estimates from MDPH’s Injury Surveillance Program indicate that in 2009 there were 36,039 nonfatal cases of opioid-related abuse, dependence, poisonings, and overdoses in Massachusetts.10
- From 1997 to 2007, the rates of opioid-related inpatient hospital discharges increased from 151.3 to 279.3 per 100,000.11
- From July 2006 through June 2007, there were 18,015 nonfatal opioid-related hospital discharges among Massachusetts residents.
- In the period June 2006 through July 2007, total charges for inpatient hospitalizations associated with opioid dependence, abuse, and/or overdose exceeded $239 million.
From 2000 to 2012, the number of unintentional opioid-related poisoning deaths (including those with undetermined intent) increased from 338 to 668.The number of confirmed cases of unintentional opioid-related poisoning deaths through December 18, 2014 was 868 – a 30% increase over 2013. It is estimated that the final number for 2013 will be 983 cases – a 47% increase.12
The Opioid-related events data from Massachusetts 2000-2010 lists opioid-related fatal overdoses and acute care hospital events associated with nonfatal opioid poisoning among Massachusetts residents from 2010 to 2012 (a three-year average). An average of 4,495 opioid-related events were reported per year. The cities with the greatest number of events were Boston (553 events), Worcester (196), New Bedford (152), Fall River (149), and Quincy (125).
Massachusetts Overdose Prevention Strategy
The state of Massachusetts is implementing a comprehensive opioid overdose prevention strategy driven by three overarching goals.13
Goal 1: Reduce the incidence of fatal and non-fatal overdose, and prevent overdoses from occurring
- Expand community-based prevention programs
- Increase the number of drug users accessing and remaining in treatment
- Assist drug users and those who serve them in reducing their risk of overdose and increasing their awareness of overdose and its consequences
- Increase the timeliness and specificity of overdose data
Goal 2: Improve the management of overdose if it occurs
- Enhance efforts of drug users, families, providers, first responders, and others to identify and manage an overdose
- Diminish real or perceived barriers to contacting emergency services in the event of an overdose
- Continue to increase the knowledge base of proven overdose management strategies
Goal 3: Reduce the amount of misused, abused, and diverted prescription opioids
- Educate prescribers on safe opioid prescribing practices and develop better mechanisms for opioid dispensing
- Educate patients and consumers on safe storage and disposal of prescription medications and potential consequences of misuse or abuse of prescription opioids
- Expand the state’s ability to monitor and track prescription opioids
New Massachusetts Department of Public Health (MDPH) Programs
As part of its opioid overdose prevention strategy, MDPH is implementing several programs:
- Overdose prevention materials: MDPH’s Bureau of Substance Abuse Services (BSAS) has developed a set of educational materials about opioid overdose prevention, which are distributed free of charge within Massachusetts. The materials are available from the Massachusetts Health Promotion Clearinghouse.
- Office-Based Opiate Treatment Programs (OBOT): With funding from BSAS, health care centers across the state are conducting OBOT programs, which provide detoxification and maintenance treatment to opioid-addicted individuals in an office-based setting, usually a physician’s office. Patients receive prescriptions for buprenorphine (Suboxone®), which they fill at local pharmacies and self-administer on a daily basis. The programs also offer integrated medical and addiction care.
- SPHERE training: BSAS partnered with the Statewide Partnership for HIV Education in Recovery Environments (SPHERE), an HIV/AIDS capacity-building project, to provide opioid overdose prevention training and technical assistance to health and human services providers in the Commonwealth. SPHERE maintains an online opioid overdose prevention page.
- Narcan distribution pilot: This program provides overdose education and intra-nasal naloxone (marketed as Narcan) distribution in various community-based settings. Program sites train potential bystanders on how to recognize signs of an overdose, take the recommended actions, and administer intra-nasal naloxone. Between December 2007 and September 2011, these sites trained more than 10,000 potential bystanders and documented more than 1,100 opioid overdose reversals.13
- ED SBIRT: Research has shown that up to 60 percent of U.S. trauma center patients test positive for one or more intoxicants. Screening and Brief Intervention and Referral to Treatment in Emergency Departments (ED SBIRT) takes advantage of teachable moments, when people can often make a clear connection between their unhealthy use and their need for emergency treatment. ED SBIRT uses a survey of patients’ health and safety needs as the basis for detecting substance misuse. Since August 2007, Health Promotion Advocates have implemented the ED SBIRT model in seven hospital EDs in Massachusetts.*
More information on these efforts is available from the MDPH website (http://www.mass.gov/eohhs/gov/departments/dph/programs/substance-abuse/prevention/opioid- overdose-prevention.html).
Massachusetts Opioid Abuse Prevention Collaborative
With funding from SAMHSA, BSAS is providing grants to municipalities (cities and towns) to address the issue of opioid misuse and abuse in the state. Started in 2013, the Massachusetts Opioid Abuse Prevention Collaborative (MOAPC) supports the implementation of local policy, practice, systems, and environmental change for three key purposes:
- To prevent the misuse of opioids (including first use)
- To prevent and reduce unintentional deaths and nonfatal hospital events associated with opioid poisonings
- To increase both the number and the capacity of municipalities across the Commonwealth addressing these issues
MOAPC emphasizes the integration of SAMHSA’s SPF model into overall prevention systems to ensure a consistent data-driven planning process across the Commonwealth, focused on implementing effective and sustainable strategies and interventions. The leading municipalities must work in partnership with neighboring municipalities, thereby forming a cluster.
Click here to see more information about the MOAPC grant and grantees.
*Note: The project has screened more than 38,530 patients, 10,627 of whom received a brief intervention on site, 8,047 of whom received a referral for further assessment or treatment. On October 17, 2011, the model we are using in Massachusetts—the Boston Medical Center and BU School of Public Health BNI ART Institute’s Project ASSERT ED SBIRT model—was included in SAMHSA’s National Registry of Evidence‐based Practice Program (http://nrepp.samhsa.gov/ViewIntervention.aspx?id=222). More information about the ED SBIRT program can be found on the MDPH website (www.mass.gov/dph/bsas); click on “Prevention Information” and then click on “Screening, Brief Intervention and Referral to Treatment.”