“The Centers for Disease Control and Prevention has classified prescription drug abuse as an epidemic. While there has been a marked decrease in the use of some illegal drugs like cocaine, data from the National Survey on Drug Use and Health (NSDUH) show that nearly one-third of people aged 12 and over who used drugs for the first time in 2009 began by using a prescription drug non-medically.
Some individuals who misuse prescription drugs, particularly teens, believe these substances are safer than illicit drugs because they are prescribed by a healthcare professional and dispensed by a pharmacist. Addressing the prescription drug abuse epidemic is not only a top priority for public health, it will also help build stronger communities and allow those with substance abuse disorders to lead healthier, more productive lives,” says the White House’s Office of National Drug Control Policy.
Below we examine the definition of the non-medical use of prescription drugs (NMUPD), what some of the commonly diverted medications are, the current trends in use nationally and in Massachusetts, the physical and psychosocial consequences of NMUPD, and where people are accessing prescription drugs.
- Definition of NMUPD
- Commonly Diverted Medications
- Estimates of Lifetime NMUPD
- Estimates of Past-Year NMUPD
- Estimates of Current NMUPD
- Initiation of Use
- Physical Consequences of NMUPD
- Psychosocial Consequences of NMUPD
There is no single agreed-upon definition of NMUPD in the scientific literature. Terms used to describe this phenomenon include prescription drug misuse, prescription drug abuse or dependence, and misuse of prescription psychotherapeutics.1, 2, 3 National health and behavioral health surveys use slightly different definitions:
- SAMHSA’s National Survey on Drug Use and Health (NSDUH) defines NMUPD as the use of a prescription drug without a prescription from a physician or simply for the experience or feeling the drug caused).4
- Both Monitoring the Future5 and CDC’s Youth Risk Behaviors Surveillance survey6 define NMUPD as the use of a prescription drug without a doctor’s prescription.
The following definition, which is somewhat broader in scope and doesn’t imply a specific reason for the misuse or pattern of misuse, tends to be more in line with the breadth and intent of current prevention initiatives within the state:
NMUPD is the intentional or unintentional use of a prescribed medication in a manner that is contrary to directions, regardless of whether a harmful outcome occurs.7
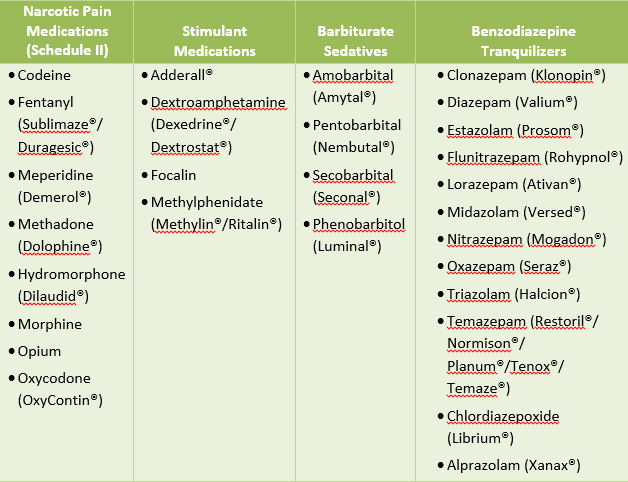
NMUPD is often broken down into four categories: pain relievers, stimulants, tranquilizers, and sedatives:4
- Pain relievers, also known as opioid analgesics or opioids, are commonly prescribed for the management of acute or chronic pain, including post-surgical pain.
- Stimulants are frequently prescribed for attention deficit hyperactivity disorder (ADHD), narcolepsy, or depression that does not respond to typical medication.
- Tranquilizers and sedatives both fall under the category of central nervous system depressants. These classes of drugs are commonly prescribed for sleep problems (e.g., insomnia), anxiety, panic disorders, and seizure disorders.
Data from the most recent NSDUH indicate that of these four categories, pain relievers (opioids) are the most commonly misused and abused type of prescription drug, far exceeding the misuse and abuse of stimulants, tranquilizers, and sedatives.
The term opioid designates a class of drugs derived from opium or manufactured synthetically with a chemical structure similar to opium. Heroin is a naturally derived opioid. Other opioids—including oxycodone (OxyContin®), morphine, meperdine, methadone, and codeine—are used therapeutically for the management of pain and other conditions. These products may be diverted from pharmaceutical purposes and used illicitly, and they have a high potential for abuse because they create psychological or physical dependence.8
(Trade names appear in parentheses.)
Estimates of Lifetime NMUPD - National
SAMHSA’s National Survey on Drug Use and Health (NSDUH) provides one of the best population-level snapshots of prescription drug misuse and abuse at the national level among civilian, non-institutionalized individuals 12 years of age or older. The most recent NSDUH results, which cover the 2014 implementation, were released in September 2015.
NSDUH asks about four types of prescription drugs: pain relievers, stimulants, tranquilizers, and sedatives. Respondents are asked to report on use without a prescription or use simply for the feeling caused by the drug.
According to 2014 NSDUH estimates:9
- A total of 130.3 million individuals ages 12 and older (49.2% of the civilian, non-institutionalized individuals in the United States) consumed an illicit drug at least once in their lifetime
- Among these individuals, 117.2 million (44.2%) reported lifetime use of marijuana, and 54.4 million (20.5%) reported non-medical lifetime use of psychotherapeutics
- Of individuals in the latter group, it is estimated that 36 million people age 12 or older (13.6%) misused pain relievers in their lifetime
- 24.8 million people age 12 or older (9.4%) misused tranquilizers, 22.5 million (8.5%) misused stimulants, and 7.8 million (3%) misused sedatives
- Within the pain reliever category, it is estimated that 7 million individuals (2.7%) specifically misused OxyContin
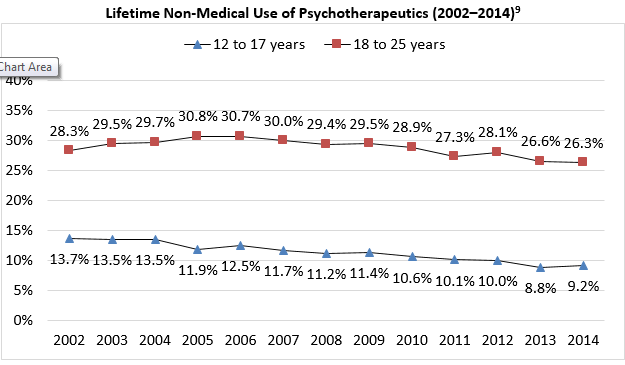
- Lifetime non-medical use of psychotherapeutics ranged from 9.2% among 12–17 year olds to 26.3% among 18–25 year olds.
- Non-medical use among 18–25 year olds peaked in 2005 at 30.8%
The 2014 survey marked the lowest reported lifetime use on record among this age group.
Similarly, lifetime non-medical use of psychotherapeutics among 12–17 year olds, which peaked in 2002 at 13.7%, was down to 8.8% in 2013—the lowest reported lifetime use among this age group. This rebounded in 2014 to 9.2%, but still marked the second lowest rate of reported lifetime misuse in 13 years.9
Additional national data are available from the Monitoring the Future (MTF) survey. MTF estimates lifetime non-medical use of psychotherapeutics among 12th-graders at 21.2% in 2012, 21.5% in 2013, 19.9% in 2014, and 18.3% in 2015, indicating a downward trend in lifetime use in recent years. Broken down by type of prescription drug, MTF found lifetime use rates among 12th-graders at 10.8% for stimulants, 8.4% for pain relievers, 6.9% for tranquilizers, and 5.9% for sedatives.5
Estimates from CDC’s Youth Risk Behaviors Surveillance survey place lifetime NMUPD in 2013 at 17.8% among public and private high school students (grades 9–12) across the country.6
Estimates of Lifetime NMUPD - Massachusetts
At the state level, the Massachusetts Youth Health Survey (MYHS), funded by DPH, provides selected data on NMUPD.
Note: The data points listed below are from the 2013 survey, as the report on the 2015 survey was not available at the writing of this document.
The MYHS estimates the following:
- Lifetime NMUPD at 3.9% among Massachusetts middle school students (grades 6–8), and 13.4% among high school students (grades 9–12)
- Lifetime misuse of prescription narcotics at 1.3% among middle-schoolers, and 5.5% among high-schoolers
- Lifetime misuse of Ritalin or Adderall at 0.8% among middle-schoolers, and 5.9% among high-schoolers
- Lifetime misuse of other prescription drugs at 2.9% among middle-schoolers, and 7.5% among high-schoolers10
Changes in the wording of these items between the 2011 and 2013 implementations limit the ability to examine trends in lifetime misuse.
Estimates of Past-Year NMUPD - National
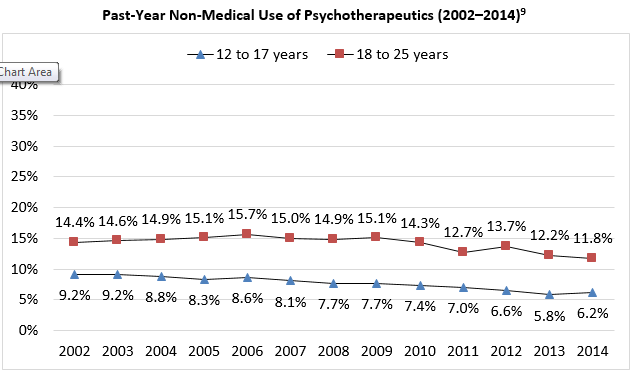
- Past-year non-medical use of psychotherapeutics in the 2014 National Survey on Drug Use and Health (NSDUH) ranged from 6.2% among 12–17 year olds to 11.8% among 18–25 year olds.
- Non-medical use of psychotherapeutics among 18–25 year olds peaked in 2006 at 15.7%; the 2014 NSDUH marked the lowest reported past-year use on record among this age group.
- Past-year non-medical use of psychotherapeutics peaked in 2003 among 12–17 year olds at 9.2%, and the 2013 NSDUH marked the lowest reported lifetime use among this age group (5.8%).
- This rebounded in 2014 to 6.2%, but still marked the second lowest rate of reported past-year misuse in 13 years.9
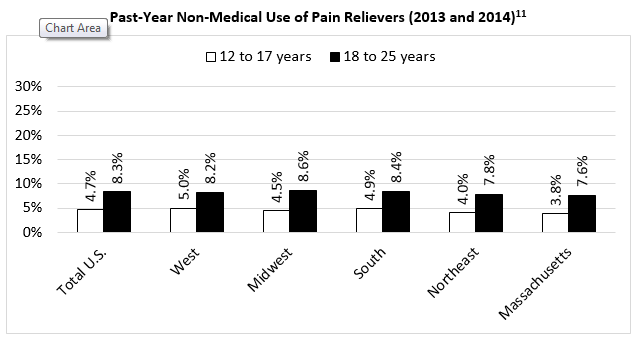
Within NSDUH’s psychotherapeutic category, pain relievers were the most prominent type of prescription drug misused, with past-year misuse rates of 4.7% among 12–17 year olds, and 7.8% among 18–25 year olds.
Past-year misuse rates of other prescription drugs:
- Tranquilizers: 1.7% among 12–17 year olds; 4.1% among 18–25 year olds
- Stimulants: 1.5% among 12–17 year olds; 3.9% among 18–25 year olds
- Sedatives: 0.5% among 12–17 year olds; 0.4% among 18–25 year olds
Past-year misuse of OxyContin was 0.7% among 12–17 year olds and 1.2% among 18–25 year olds.9
Monitoring the Future (MTF) estimates past-year non-medical use of psychotherapeutics among 12th-graders at 14.8% in 2012, 15% in 2013, 13.9% in 2014, and 12.9% in 2015, indicating a downward trend in past-year use in recent years.
Broken down by type of prescription drug, MTF found past-year use rates among 12th-graders at 7.7% for stimulants, 5.4% for pain relievers, 4.7% for tranquilizers, and 3.6% for sedatives.
Sub-divided even further, MTF estimates past-year misuse among 12th-graders at 7.5% for Adderall, 2% for Ritalin, 4.4% for Vicodin, and 3.7% for OxyContin.5
Estimates of Past Year NMUPD - Massachusetts
Limited data on past-year misuse of prescription drugs at the state level are available from the 2014 National Survey on Drug Use and Health (NSDUH), which aggregates two years of data together. The 2013 and 2014 pooled estimate from NSDUH indicates that 3.8% of individuals 12–17 years of age and 7.6% of individuals 18–25 years of age in Massachusetts misused prescription pain relievers in the past year.
The estimate for Massachusetts is slightly lower than the rest of the Northeast in past-year misuse of prescription pain relievers, and the estimate for the Northeast region is lower than for other regions of the country.11
Estimates of Current NMUPD - National
Past-month non-medical use of psychotherapeutics in the 2014 NSDUH ranged from 2.6% among 12–17 year olds to 4.4% among 18–25 year olds.
Non-medical use among 18–25 year olds peaked in 2006 at 6.5% and has been lower than that rate in each successive year—the 2014 survey marked the lowest reported use on record among this age group.
Similarly, non-medical use of psychotherapeutics peaked in 2002 and 2003 among 12–17 year olds at 4.0% and has been lower than that rate in each successive year.
The 2013 survey marked the lowest reported use among this age group (2.2%). This rebounded in 2014 to 2.6%, but still marked the second lowest rate of reported misuse in 13 years.9
Within the psychotherapeutic category, pain relievers were the most prominent type of prescription drug misused, with past-month misuse rates among 12–17 year olds of 1.9%, and among 18–25 year olds of 2.8%.
Past-year misuse rates of other prescription drugs:
- Stimulants: 0.7% among 12–17 year olds; 1.2% among 18–25 year olds
- Tranquilizers: 0.4% among 12–17 year olds; 1.2% among 18–25 year olds
- Sedatives: 0.2% among both 12–17 year olds and 18–25 year olds
Past-month misuse of OxyContin was 0.1% among 12–17 year olds and 0.3% among 18–25 year olds.9
Past-month misuse of pain relievers was second only to marijuana among the specific illicit drugs measured by the survey (CBHSQ, 2015).
Monitoring the Future (MTF) estimates past-month non-medical use of psychotherapeutics among 12th-graders at 7% in both 2012 and 2013, 6.4% in 2014, and 5.9% in 2015, indicating a downward trend in past-month use in recent years.
Broken down by type of prescription drug, MTF found past-year use rates among 12th-graders at 3.2% for stimulants, 2.1% for pain relievers, 2% for tranquilizers, and 1.7% for sedatives.5
Estimates of Current NMUPD - Massachusetts
At the state level, the Massachusetts Youth Health Survey estimated in 2013 that 2% of middle school students and 3% of high school students engaged in NMUPD in the past 30 days.10
- In 2014, 2.1 million individuals age 12 or older initiated NMUPD.9
- Among those ages 12–17, there were 641,000 initiates (2.6% of this age group).9
- Among those ages 18–25, there were 884,000 new initiates (2.5% of this age group).9
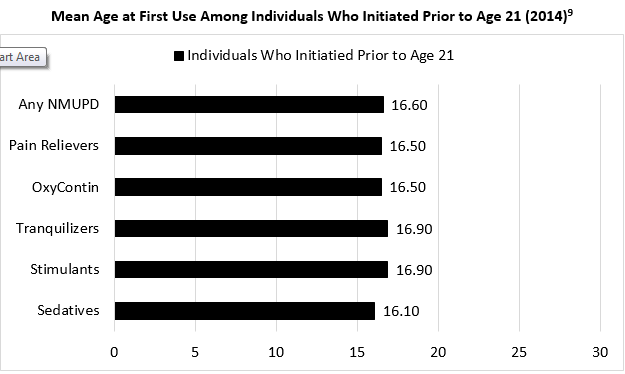
- Among individuals who initiated use prior to turning 21 years of age, the average age of onset was 16.6 years, with minor variation by type of psychotherapeutic.9
- In a longitudinal study of adolescents from grade 10 through age 20, the majority (69.5%) of participants who used prescription drugs non-medically reported starting use in high school.12
Physical Consequences of NMUPD
- Acute Side Effects of Medication and Withdrawal Symptoms
- Dependence
- Increased Risk of Overdose, Injury, and Death
Acute Side Effects of Medication and Withdrawal Symptoms
Prescription drugs all have potential acute side effects that range from mild symptoms to more severe reactions that can lead to significant morbidity and, potentially, death. Effects vary by the type of medication misused.
- Common acute side effects of opioid prescription drugs include nausea, sedation or drowsiness, depressed respiration, euphoria, dysphoria, constipation, and itching.
- Termination of or reduction in opioid use can lead to withdrawal symptoms, including restlessness, muscle and bone pain, insomnia, diarrhea, vomiting, cold flashes with goose bumps, and involuntary leg movements.13, 14
- Side effects of central nervous system (CNS) depressants (e.g., sedatives, tranquilizers) include increased drowsiness or sedation. CNS depressants can slow heart rate and respiration when combined with prescription pain medications, some types of over-the-counter cold or allergy medications, or alcohol. 14
- Rapid discontinuation of sedatives or tranquilizers can lead to seizures, some of which can be life-threatening.14
- Effects of stimulant medications include increases in alertness, attention, and energy; physiological effects also include elevated heart rate and blood pressure, increased respiration, suppressed appetite, and sleep deprivation.14
- Frequent use of stimulants during a short period of time can lead to feelings of hostility or paranoia. Large doses can lead to irregular heartbeat and high body temperature, as well as the potential for heart failure or seizures.14
- Stimulant withdrawal symptoms can include fatigue, depression, and disrupted sleep cycles.14
Other adverse consequences associated with regular NMUPD over a long period of time include hormonal and immune system effects, physiological dependence, and increased sensitivity to pain, all of which can lead to an increase in physical disability.13
NMUPD is associated with a greater likelihood of developing dependence,1, 15, 16 particularly for adolescents who begin use early. Opioid analgesics, which are in the pain reliever category of prescription drugs, are more likely to lead to dependence.
National survey data suggest that adolescent females may be at greater risk of dependence on prescription drugs compared to their male counterparts. There are several hypothesized reasons for this difference, including potentially greater pharmacologic sensitivity in females, and that females are more likely to be prescribed medications, thus giving them greater access to prescription drugs.17
Increased Risk of Overdose, Injury, and Death
It is well-documented that NMUPD, particularly misuse of narcotic pain relievers, is associated with an increase in the number of emergency department (ED) visits. Between 1972 and 2011, the Drug Abuse Warning Network (DAWN) tracked drug-related ED visits in the United States.
Though the DAWN surveillance system is in the process of being replaced by the National Hospital Care Survey, SAMHSA’s Center for Behavioral Health Statistics and Quality continues to analyze the DAWN dataset through 2011:
- In the final year of DAWN, 1,244,872 ED visits involved NMUPD, 366,181 (29%) of which involved narcotic pain relievers—mostly oxycodone (12.1%), hydrocodone (6.6%), and methadone (5.4%).
- This constituted an increase of 117% (from 168,379 to 366,181) between 2005 and 2011, although there was evidence of a stabilization in trend between 2008 and 2011 (Crane, 2015).
CDC and the Commonwealth of Massachusetts have each launched websites devoted to tracking drug-related overdose deaths. According to the CDC:18
- Drug overdose was the leading cause of injury death in 2013, resulting in 43,982 fatalities nationwide.
- Among young adults and adults (ages 25–64), deaths from drug overdose exceeded the number of deaths from motor vehicle fatalities.
- Breaking down these numbers a little further, roughly half the drug overdose deaths in 2013 (52%) were related to prescription drugs (22,767 cases).
- Within this group, almost three-quarters (71%) involved opioid pain relievers, and one-third (31%) involved benzodiazepines.
The CDC estimates that 44 people die each day as a result of prescription opioid overdose. Among this sub-group, those most likely to experience a fatality were between the ages of 25 and 54, non-Hispanic whites, and male.18
Within Massachusetts, DPH confirmed 1,099 opioid overdose fatalities in 2014 of unintentional or undetermined intent and estimates an additional 61–89 cases once unresolved cases have been finalized. Based on the confirmed cases alone, this constitutes a 65% increase over the number of opioid overdose fatalities observed in 2012 (n = 668).
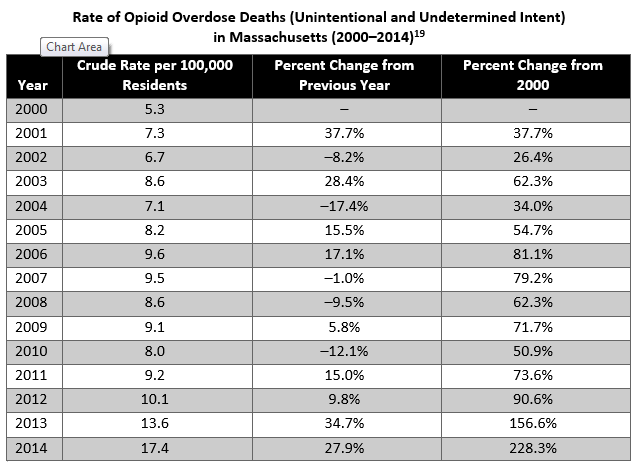
During 2014:19
- The unintentional and undetermined intent opioid overdose death rate (including heroin deaths) was estimated at 17.4 people per 100,000).
- This constitutes a 228% increase from the observed death rate in 2000 (5.3 per 100,000) and a 28% increase from the observed death rate in 2013 (13.6 per 100,000).
- On a year-to-year basis, the death rate has increased in 9 of the past 14 years, with small reversals in 2002, 2004, 2007, 2008, and 2010.
- The death rate has increased every year since 2010, which is the longest period of uninterrupted growth since 2000.
Psychosocial Consequences of NMUPD
Association with Psychiatric Conditions
NMUPD is associated with increased risk of developing psychiatric and other medical conditions,20, 21 including depression, anxiety, ADHD, and mania:
- Hall, Howard, and McCabe22 found that among a sample of 723 adolescents in residential care for antisocial behavior, those who reported high levels of anxiety and depression also reported significantly greater amounts of sedative/anxiolytic misuse compared to adolescents who did not report high levels of anxiety and depression.
- Several studies have demonstrated a link between major depressive disorder and greater rates of NMUPD;13, 23, 24, 25 however, it is unknown if this indicates a directional relationship or whether another factor might account for both conditions.
- Research has found an association between illicit drug use and increased risk of suicide; however, suicide risk has not been directly linked with NMUPD.26
- A study of treatment-seeking, opiate-dependent adolescents found that prescription drug opioid users reported higher rates of ADHD and manic episodes than did adolescent heroin users. Both groups of adolescents reported high scores on a measure of depression.25
Additional research is needed to determine whether certain classes of prescription drugs are related to different types of psychiatric or other medical conditions.
Delinquency and/or Violent Behavior
Several studies have demonstrated a link between violent or delinquent behavior and NMUPD.12, 22, 27, 28, 29 The direction of the relationship (i.e., whether NMUPD leads to increased violent or delinquent behavior, or whether delinquent behavior leads to future NMUPD) has not been established. However, in a longitudinal study of adolescents assessed from grade 10 to age 20, the only unique predictor of non-medical opiate prescription drug use was violent behavior. This relationship remained significant after accounting for licit (alcohol, tobacco) and illicit (marijuana, cocaine/crack, psychedelics, heroin) drug use.12
Greater misuse of prescription drugs is associated with lower levels of educational attainment.27 Adolescents reporting greater rates of NMUPD also demonstrate poorer academic performance24, 30 and a greater likelihood of school dropout.23, 31 Due to the cross-sectional design of these research studies, it is not possible to rule out that poorer academic functioning occurs prior to the onset of NMUPD or that another factor is associated with both academic functioning and NMUPD.