Cultural competence, which also includes linguistic competence, must be considered at each step of the SPF model. Cultural and linguistic competence help to ensure that the needs of all community members are identified and addressed, thereby contributing to the effectiveness of your strategies. Your group should incorporate cultural and linguistic competence into every step of the SPF.
- What Is Cultural Competence?
- What Is Linguistic Competence?
- Why Cultural and Linguistic Competence Matter
- National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care (National CLAS Standards)
Cultural competence is the ability of an individual or organization to interact effectively with people from different cultures. Developing cultural competence is an evolving, dynamic process that takes time and occurs along a continuum.31 For your efforts to prevent or reduce substance misuse and abuse to be effective, you must understand the cultural context of your target community and have the required skills and resources for working within this context.
Although some people may think of culture solely in terms of race or ethnicity, there are many other elements to consider, such as age, educational level, socioeconomic status, gender identity, language(s), and cognitive and physical abilities and limitations.38 You must be respectful of and responsive to the health beliefs, practices, and cultural and linguistic needs of the diverse population groups in your target community. This means learning more about the community; drawing on community-based values, traditions, and customs; and working with persons from the community to plan, implement, and evaluate your strategies.
What Is Linguistic Competence?
Linguistic competence involves more than having bilingual staff; it refers to the ability to communicate with a variety of different cultural groups, including people with low literacy, non-English speakers, and those with disabilities. The National Center for Cultural Competence defines linguistic competence as follows:
The capacity of an organization and its personnel to communicate effectively, and convey information in a manner that is easily understood by diverse audiences including persons of limited English proficiency, those who have low literacy skills or are not literate, individuals with disabilities, and those who are deaf or hard of hearing. Linguistic competency requires organizational and provider capacity to respond effectively to the health and mental health literacy needs of populations served. The organization must have policy, structures, practices, procedures, and dedicated resources to support this capacity. (p. 1)40
The National Center for Cultural Competence39 identifies the following guiding values and principles for language access:
- Services and supports are delivered in the preferred language and/or mode of delivery of the population served
- Written materials are translated, adapted, and/or provided in alternative formats based on the needs and preferences of the populations served
- Interpretation and translation services comply with all relevant federal, state, and local mandates governing language access
- Consumers are engaged in evaluation of language access and other communication services to ensure quality and satisfaction
You might consider some or all of the following approaches:
- Hiring bilingual/bicultural or multilingual/multicultural staff
- Providing foreign language interpretation services
- Printing materials in easy-to-read, low-literacy, picture, and symbol formats
- Offering sign language interpretation services
- Using TTY and other assistive technology devices
- Offering materials in alternative formats (e.g., audiotape, Braille, enlarged print)
- Adapting how you share information with individuals who experience cognitive disabilities
- Translating legally binding documents (e.g., consent forms, confidentiality and patient rights statements), signage, health education materials, and public awareness materials and campaigns
- Using media targeted to particular ethnic groups and in languages other than English (e.g., television, radio, Internet, newspapers, periodicals)
Why Cultural and Linguistic Competence Matter
Consider the following examples:
- A community group wants to educate parents of high school students on the risks of underage alcohol consumption. As Spanish is the primary language of many parents, the group asks a teacher to translate the take-home flyer. However, the teacher’s translation does not use vocabulary and idioms that match the parents’ ethnicity, so families don’t read it or don’t understand it, and some are even offended by it.
The flyer is then revised based on input from a small group of parents. It is now much more clear and useful to the school’s Spanish-speaking families.
- To reduce alcohol misuse, a community group hires professional outreach workers to deliver messages to friends, family members, and individuals who are misusing alcohol. However, the professionals don’t connect well with the people they are trying to educate. The group then recruits members of the community who are in recovery, and trains them to deliver outreach education. This strategy has much greater success.
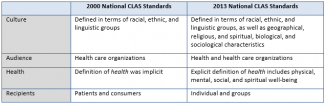
The National CLAS Standards are a comprehensive series of guidelines that inform, guide, and facilitate practices related to culturally and linguistically appropriate health services.38 Originally developed by the HHS Office of Minority Health in 2000, the standards were updated in 2013 after a public comment period, a systematic literature review, and input from a National Project Advisory Committee.
The standards have been updated and expanded to address the importance of cultural and linguistic competence at every point of contact throughout the health care and health services continuum. Here are some of the main differences between the 2000 and 2013 National CLAS Standards:41
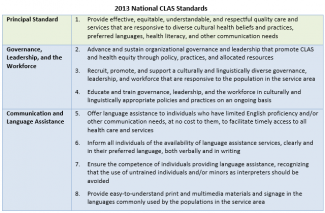
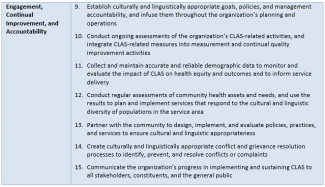
The 15 standards are organized into one Principal Standard and three themes:
Resources for implementing the National CLAS Standards are available from the Office of Minority Health’s Think Cultural Health website.